

18/07/2017
MERCEDES BORDA MÁS
Project Manager (University of Seville)
AGUSTÍN LUQUE FERNÁNDEZ
University of Seville
MARÍA LUISA AVARGUES NAVARRO
University of Seville
MILAGROSA SÁNCHEZ MARTÍN
Loyola University of Andalucía
MARÍA DEL ROSARIO RAMÍREZ CASTRO
SPA-FREMAP
MACARENA PÉREZ HIDALGO
SPA-FREMAP
FRANCISCO JAVIER NIETO LORITE
University of Seville
MARÍA ÁNGELES PÉREZ SAN GREGORIO
University of Seville
AGUSTÍN MARTÍN RODRÍGUEZ
University of Seville
MARÍA DEL MAR BENÍTEZ HERNÁNDEZ
University of Seville
NEREA MARÍA ALMEDA MARTÍNEZ
University of Seville
The general objective was to analyze the relationship that exists between occupational stress, emotional eating, abnormal eating patterns, and health by studying 407 workers from the University of Seville. To do this, the survey “Estrés laboral y comer emocional” (Occupational Stress and Emotional Eating) was planned, written, and validated. Its psychometric properties are good.
The most relevant conclusions are:
There is a significant percentage of overweight and obese people, with a greater portion being obese. This rate is higher for men and for non-teaching staff.
The most frequently mentioned stressor related to the work environment was the demands of work and how it is organized, with higher percentages among men and teaching staff.
Negative emotions felt in stressful situations in the work environment tend to affect the eating habits of both men and women, as well as both teaching and non-teaching staff. Those that try and “eat” their negative feelings find that their mood is affected, with emotions associated with anxiety.
A slightly higher percentage of women eat late at night, almost compulsively eat a food, and snack throughout the day. Men only had a higher percentage when it came to binge eating. Non-teaching staff had a slightly higher percentage for these four types of unhealthy patterns.
The most frequent physical health problems were musculoskeletal, digestive, and cardiovascular problems, as well as being overweight or obese. Organizational and personal measures are laid out for promoting healthy work environments and habits in the university community. These adapted environments and habits would help prevent occupational stress, emotional eating, obesity, and overweight, as well as other associated health problems.
The term occupational stress refers to the imbalance or discomfort that a worker experiences due to factors or demands related to work. This imbalance produces a change in the body that can affect the worker’s physical and mental health in ways both big and small.
Often the work environment is associated with emotions like sadness, worry, frustration, or anger that are provoked by certain conditions in a work context. These sources of stress are considered subjective psychosocial risk factors that can lead to occupational stress, understood to be a psychosocial risk factor itself, with significant effects on the health of workers. Out of health problems that lead to having to take at least two weeks off from work, stress and emotional problems were the cause a quarter of the time. In fact, stress related to work has now become the second most common health problem among workers, as much as 28% of workers experiencing these problems.
From a behavioral point of view, notable consequences or effects of occupational stress include an increased rate of tobacco and alcohol use and changes in eating habits, that is to say “eating poorly”.
“Emotional eating” (or emotional hunger) is the tendency to consume food as a response to negative emotions, more as a way to deal with negative feelings rather than as a way to satisfy hunger. Habits of consumption manifest themselves differently between these two forms of hunger (see Table 1).
Tabla 1. Características del hambre emocional y hambre física.
| Hambre emocional | Hambre física |
|---|---|
| Aparece de repente | Aparece gradualmente |
| Se siente como una necesidad de satisfacer al momento | Se puede esperar |
| Se ansía alimentos concretos que resulten placenteros | Se está abierto a “un montón” de cosas buenas |
| Aun con el estómago lleno, no se siente satisfecho | Se detiene cuando se está lleno |
| Se desencadenan sentimientos de culpa, impotencia y vergüenza | Comer para satisfacer el hambre física no despierta sentimientos malos hacia uno mismo |
People that eat due to negative emotions, compared to people that eat due to positive emotions, tend to show more symptoms related to eating disorders and other psychological disorders, making emotional eating a risk factor for the development of an eating disorder or obesity in the general population. However, in situations of occupational stress, women more frequently tend to resort to eating in an abnormal, uncontrolled manner, often with binges, for emotional reasons, this according to existing scientific research.
Emotions have a powerful effect on the way people eat and the types of food that they eat. Most people at one time or another have eaten an entire bag of potato chips out of worry or nervousness, or have scarfed down chocolate after having to deal with a conflict or a stressful situation. However, when this eating pattern becomes a habit, emotional eating can affect a person’s weight, health, and general well-being.
The most common eating patterns related to unhealthy dietary habits are bingeing, grazing, late-night eating, and food addiction. Maintaining these habits is associated with health problems.
The most relevant aspects of these patterns are the following:
Bingeing: also called “compulsive over-eating”, “insatiable appetite”, or “uncontrolled eating”. Bingeing involves eating large amounts of food (which are usually “forbidden foods” that are avoided in the person’s normal diet) in a period of time associated with or brought about by emotional factors (such as anxiety, tenseness, dissatisfaction, frustration, etc.), with feelings of lacking self-control, ending when the person “feels full”. This pattern of consumption is typically done alone because of the shame it makes the person feel. At the same time, the person feels guilt and sadness because of their lack of self-control. Often people who go through binge-eating episodes end up overweight or obese, as well as experiencing other health problems.
Grazing: an abnormal dietary pattern associated with emotions like anxiety, among others, and at times “just because”, such as out of boredom or “not having anything else to do”. Grazing involves consuming small amounts of food almost constantly, eating a variety of things. Unlike bingeing, where the person feels bad about the way that they’re eating, with grazing the person may experience pleasure and may even enjoy eating more and more over time, as they graze with less anxiety. As such, grazing tends to perpetuate itself as a “healthy” habit.
Late-night eating: an eating pattern similar to bingeing that affects approximately 1.5% of the population, with similar incidence among both men and women. It involves eating large amounts of food in the middle of the night, with the person resorting to this strategy for two reasons: mainly due to the fear of being discovered and the guilt the person feels for lacking self-control. What’s more, in addition to dietary restriction, a bad mood and stress are risk factors for this eating pattern.
Las personas con el síndrome de comer la noche suelen ser obesos o con sobrepeso, lo que los hace susceptibles a los problemas de salud causados por el exceso de peso, incluyendo la presión arterial alta, diabetes y colesterol alto, similar a las personas con atracones. En los casos de obesidad se aumenta el riesgo de enfermedades del corazón y con frecuencia presentan alteraciones del sueño.
eople with night eating syndrome tend to be obese or overweight, which makes them susceptible to health problems caused by excess weight, including high blood pressure, diabetes, and high cholesterol, similar to the problems that binge eaters face. In the case of obesity, there is a higher risk of heart disease, and obese people often have trouble sleeping.
Food addiction: this involves eating a specific food almost systematically in an amount that is not planned before the person starts eating. The person eats as if out of compulsion or “temptation”, well beyond typical eating or in an isolated way.
Some of these addictive, “tempting” foods that activate these brain circuits and produce a good feeling are chocolate, french fries, and cookies, among other things. At times of negative emotional impact, these foods tend to become “favorites” for overeating and bingeing episodes.
Clearly, “eating bad” for emotional reasons related to occupational stress can lead to health problems [1]. Anxiety and mood swings act as triggers for unhealthy eating patterns where overeating leads to becoming overweight or obese, and as a consequence, health risks appear like hypertension, cardiovascular problems, and joint pain, among other things.
Given the impact that the work environment has on people, causing stress that affects the health of workers, the World Health Organization [2] defined a healthy workplace in the following terms: “… one in which workers and managers collaborate to use a continual improvement process to protect and promote the health, safety and well-being of all workers and the sustainability of the workplace.” (p. 16). According to the WHO model, there are four areas in which to take action: the physical work environment, the psychosocial work environment, personal health resources, and the enterprise’s community involvement [3].
The university community, in its commitment to being a healthy institution that promotes learning, as well as in application of laws on psychosocial risks (Law 31/1995 of 8 November, on the Prevention of Occupational Hazards), has established objectives including decreasing physical, psychological, and environmental risk factors for students, educators, and non-teaching staff because of the significant impact on people’s learning, success, and work productivity, as well as the effects on health.
Bearing in mind that a significant portion of a person’s life is spent in the workplace, the University has made it a priority to provide the entire university community, and more specifically workers, with healthy environments that encourage improvements in lifestyle and interpersonal relations, greater productivity, and reduce absences, health risks, and spending on health.
With this established, to take action to this end, it is necessary to first identify and evaluate risks that may be associated. According to Article 16 of the previously cited Spanish Occupational Hazard Prevention Law, once this evaluation is complete, if the results show a risky situation, preventive measures necessary for eliminating or reducing and controlling the risks should be taken. Psychosocial intervention actions can be classified according to different criteria. There are different levels of action, separated into primary, secondary, and tertiary interventions.
For this reason, this study is looking at the new subject of “emotional eating” and its relation to occupational stress, a psychosocial risk factor present in the university environment, as has been found in prior studies conducted in our community [4 y 5], with the objective of analyzing the relationship that exists between occupational stress, emotional eating, abnormal eating patterns, and health for university personnel. Lastly, this study aims to help design strategies for intervention to help promote healthy work habits and environments in the university community.
Methodology
The sample was taken from two sources: 1) people going for check-ups at the Medical Office of the Department for the Prevention of Occupational Hazards, and 2) people asking for psychological counseling, either on their own or by recommendation from the Occupational Physician, from the Clinical Psychology Office of the Department for the Prevention of Occupational Hazards.
The study included the participation of 407 workers from the University of Seville, with an average age of 45.05 years (SD=8.57) (range = 23-67 years).
Out of all responses given by participants, 222 were from men (54.5%) and 177 were from women (43.5%), with a higher average age among men than among women (averageage=46.36; SD=8.41 and averageage=43.51; SD=8.48, respectively).
In regards to the category of profession, out of all responses given by workers, 57.7% (121 men -30%- and 112 women -27.7%) were administration and services personnel (ASP), or non-teaching staff, and 39.5% were teaching and research personnel (TRP) (96 men -23.8%- and 63 women -15.7%).
In regards to health indicators, one of the simplest, most reliable methods was used for determining if weight is at the right point to not pose a health risk. This indicator is known as the body mass index (BMI), which puts weight in proportion to height [BMI = weight (kg) / height2 (m)]. A BMI above 30 is considered to pose a real risk to health.
Out of all responses from participants, the average BMI was 25.23 (SD=4.46) (range: 16.40 – 48.22 kg), being higher among men (averageBMI=26.32; SD=4.11) than among women (averageBMI=23.92; SD=4.56). Non-teaching staff (ASP) also had a higher average BMI (averageASP=25.84; SD=4.95) than faculty (TRP) (averageTRP=24.31; SD=3.42).
For evaluation, the research team designed a survey specifically to measure stress and emotional eating in the university community. The survey is made up of five questions that gather different information about the person’s current situation, related to emotional eating, stress in daily life and occupational stress, abnormal eating patterns, and consequences for health associated with the work context (see Appendix 1). Its psychometric properties are good. Reliability analysis using Cronbach’s alpha showed a value of 0.92 for the 12 items, which can be considered a very satisfactory value. With the Emotional Appetite Questionnaire (EMAQ), a satisfactory correlation value of 0.70 was found (p=0.000). As such, one can conclude that there is convergent validity between the two instruments.
Results
Figure 1. Distribution of participants according to BMI and sex.
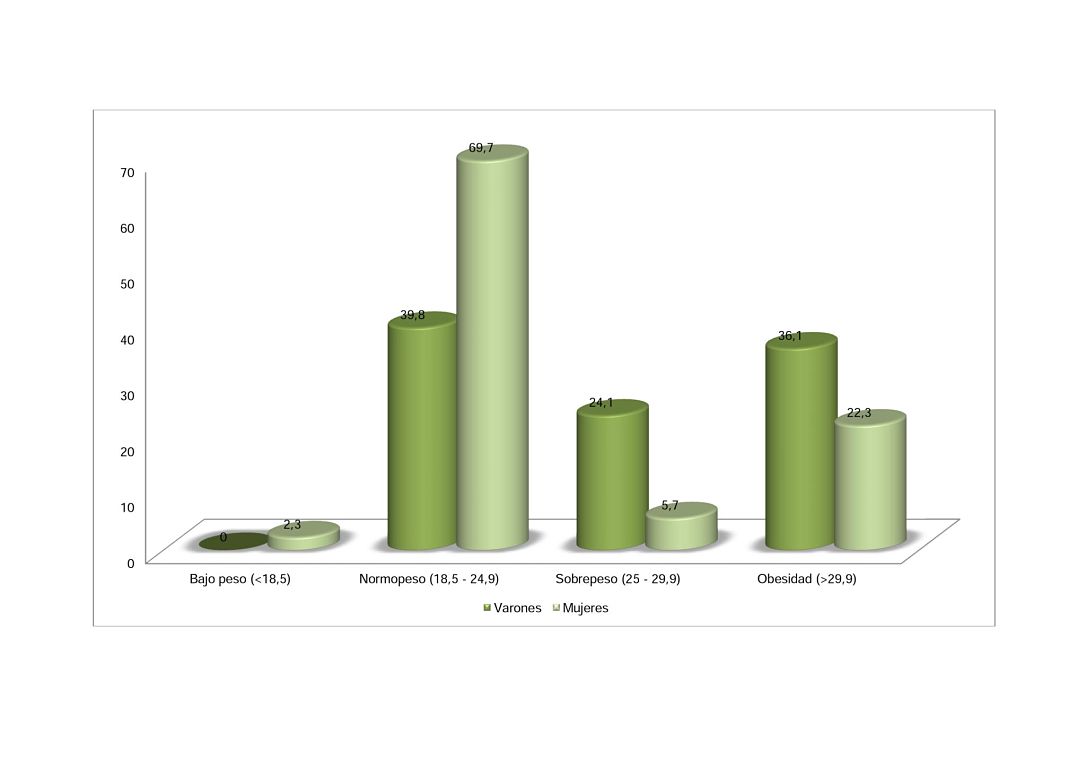
In regards to the indicator for health risk, the average BMI for all workers was 25.23 (SD=4.46) (range: 16.40 – 48.22 kg), being higher among men (BMImen=26.32; SD=4.11) than among women (BMIwomen=23.92; SD=4.56). Non-teaching staff (ASP) also had a higher average BMI (averageASP=25.84; SD=4.95) than faculty (TRP) (averageTRP=24.31; SD=3.42). The differences in means among the sexes (men and women) (t358.263=5.424; p=.000) and among profession (ASP and TRP) (t401.76=3.661; p=.000) were statistically significant for both variables.
When categorizing BMI into ranges, including underweight (<18.5), normal weight (18.5-24.9), overweight (25-29.9), and obese (>29.9), the greatest percentage of workers (53.2%) were in the normal weight range, with significant differences (X2=234.965; df=3; p=.000), with a higher percentage of normal weight people among women (69.7%) than among men (39.8%). However, it should be noted that there was a high rate of overweight and obesity (45.8%, or 15.9% and 29.9% respectively), higher among men (60.2%) than among women (28%). In other words, while more than two thirds of women had an appropriate weight in proportion to their height, almost two thirds of men were overweight or obese (see Figure 1).
When looking at BMI according to profession, the non-teaching staff had a higher percentage of overweight and obese people (44.9%) than the teaching staff (35.2%), with a greater percentage of obesity (ASP: 34.6% vs TRP=20.5%) than overweight (ASP: 10.3% vs TRP=14.3%). As such, between 35% and 45% of workers were overweight or obese, with a higher rate of obesity among non-teaching staff (see Figure 2).
Figure 2. Distribution of participants according to BMI and profession.

The first question on the survey asks if the person currently experiences stress in their daily life, considering various factors or sources of stress (see Figure 3).
As can be seen in Figure 3, nearly half of workers (49.3%) consider the work environment to be a stress factor or a source of stress,with a higher percentage among men (27.1%) compared to women (22.2%) and among faculty (TRP) (28.1%) compared to non-teaching staff (ASP) (21.1%).
Figure 3. Presence of current perceived sources of stress.
Figure 4. Presence of current perceived sources of occupational stress.
Subsequent questions go more in depth about the experience of stress in the work environment. As can be seen in Figure 4, it is worth noting that 40.9% of workers consider the organization and demands of their work to be a stress factor or source of stress related to the work environment. This percentage was higher among men (22.3%) than among women (18.6%) and among faculty (TRP) (18.8%) than among non-teaching staff (ASP) (21.3%).
Additionally, for a moderate percentage of people (26.6%), the future of their career was a current source of occupational stress, with similar percentages between women and men (13.5% vs 13.1%) and between non-teaching staff and faculty (13.4% vs 13.2%).
The survey also attempted to discern if people experience certain negative emotions in their work environment when faced with stressful situations and if, as a consequence, they changed their eating or “ate their feelings” (eating more food or less food). Breaking down the results by sex, one can see that, except when they feel anxious, the women had higher percentages for the different emotions, with a greater difference in the percentages for emotions that reflect mood. To be specific, women tend to eat more when they feel bored (40.2%), depressed (29.2%), frustrated (28.8%), and sad (23.7%). Additionally, they “eat their feelings” when they feel dissatisfied or lacking self-control (30.3% and 18.6% respectively). For both men and women, feeling nervous (30.1% vs 30%) or tense (26.7% vs 27.3%) leads them to eat more with almost identical percentages (see Figure 5).
Figure 5. Negative emotions and “eating one’s feelings” by eating more according to sex.
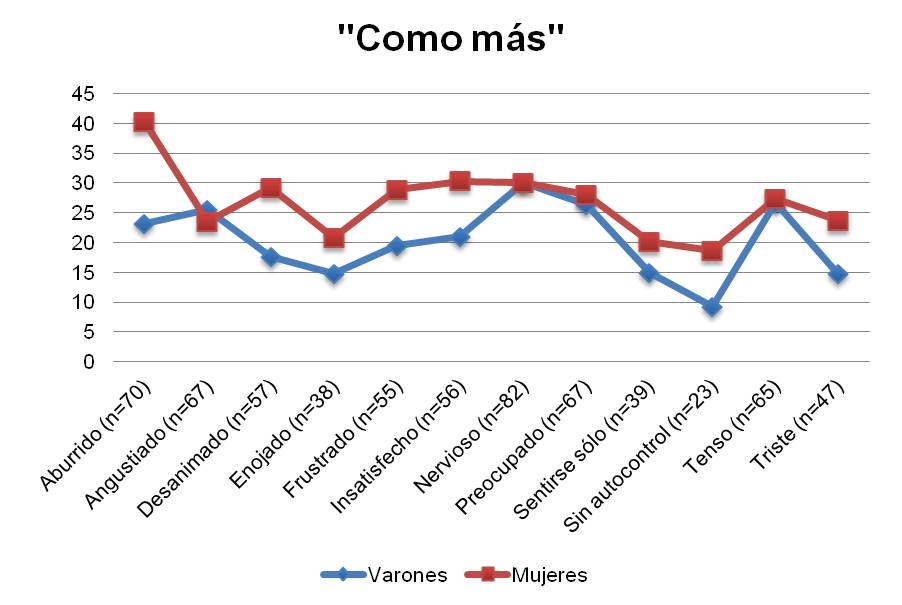
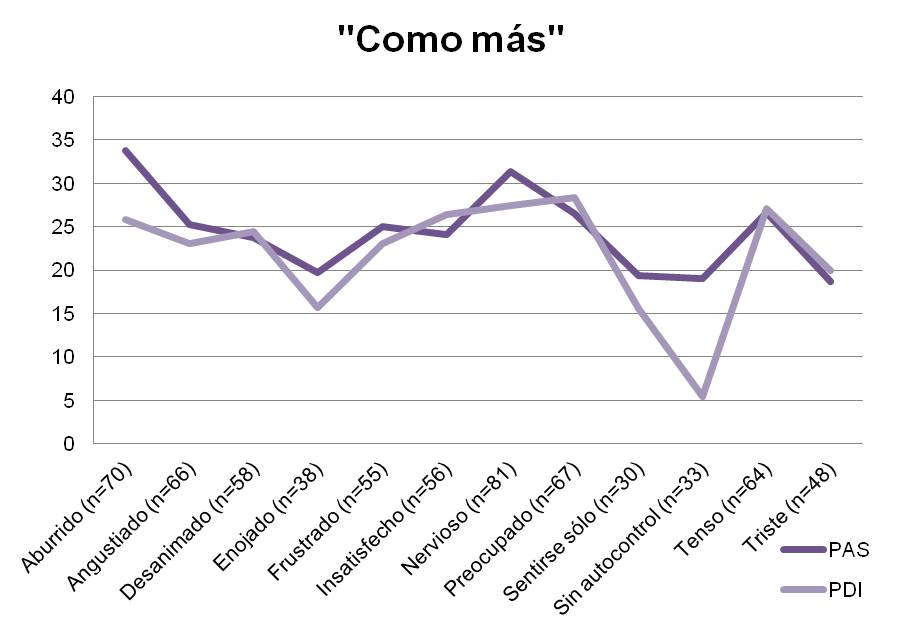
Figure 6. Negative emotions and “eating one’s feelings” by eating more according to profession.
As such, negative emotions felt in stressful situations related to the work environment tend to affect the eating habits of a significant portion of workers, both men and women, in such a way that some tend to eat less and others tend to eat more. Those that “eat their feelings” in regards to experienced uneasiness made up a moderate percentage, with a clear trend toward eating more food for emotions related to anxiety than related to depression, especially for women.
When analyzing results based on profession, meaning non-teaching personnel (ASP) versus teaching and research personnel (TRP), one can see that for both ASP and TRP emotions related to anxiety lead people to eat more. These emotions include feeling worried (26.5% vs 28.3% respectively), nervous (31.3% vs 27.4%), tense (26.6% vs 27.1%), anxious (25.2% vs 23.1%), or dissatisfied (24.1% vs 26.4%), with fairly similar and slightly higher percentages among TRP, except for nervousness and dissatisfaction. Additionally, for both non-teaching and teaching staff, emotions related to mood affected people’s eating habits, leading them to “eat their feelings”. These emotions include feeling bored (33.8% vs 25.8% respectively), with a higher percentage for ASP; also feeling depressed (23.7% vs 24.4%) and sad (18.7% vs 20%), with almost the same percentages between the groups.
One aspect of note is the significant difference between ASP and TRP in the percentage of people saying that they tend to eat more when they perceive that they have little control. For this situation, 19.8% of non-teaching staff said they eat more versus 3.1% for teaching personnel (X2=8.852; p=.012).
As such, negative emotions felt in stressful situations related to the work environment tend to affect the eating habits of a significant portion of workers, both teaching and non-teaching staff, in such a way that some tend to eat less and others tend to eat more. Those that try and “eat” their negative feelings, about one third of workers, find that they are affected by emotions associated both with anxiety and with mood.
The survey also examines the eating pattern that people use when they change their eating habits or “eat their feelings” as a result of negative emotions caused by the work environment. Of the four unhealthy eating patterns, while in this group of workers there was a significant number of workers “grazing all day”, the habit of “bingeing once or more per day” was the one that reflected a greater effect on health, as seen in the number of people that were overweight or obese (X2=40.768, p=.000). Secondly, there was the tendency to “eat a food almost compulsively” (X2=21.520, p=.000), followed by “grazing all day long” (X2=15.213, p=.000).
One can see that a slightly higher percentage of women compared to men used these unhealthy eating patterns. Such was the case for night eating (3.4% vs 2.3%), almost compulsively eating a food (15.3% vs 10.4%), and grazing all day long (37.5% vs 18.5%), with a significant difference in this last pattern (X2=7.870; p=.005). Men only had a higher percentage when it came to binge eating (9% vs 5.6%) (See Figure 7).
Figure 7. Distribution of participants according to eating pattern and sex.
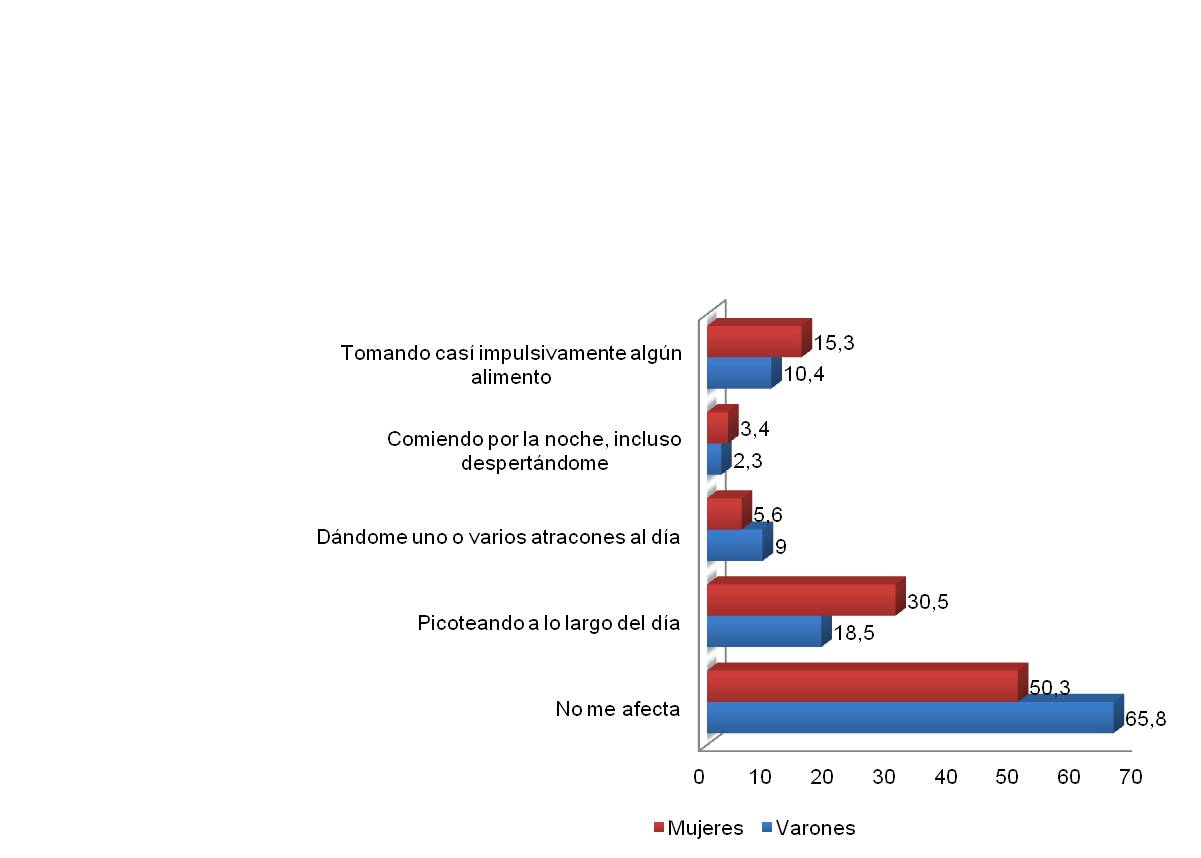
Figure 8. Distribution of participants according to eating pattern and profession.
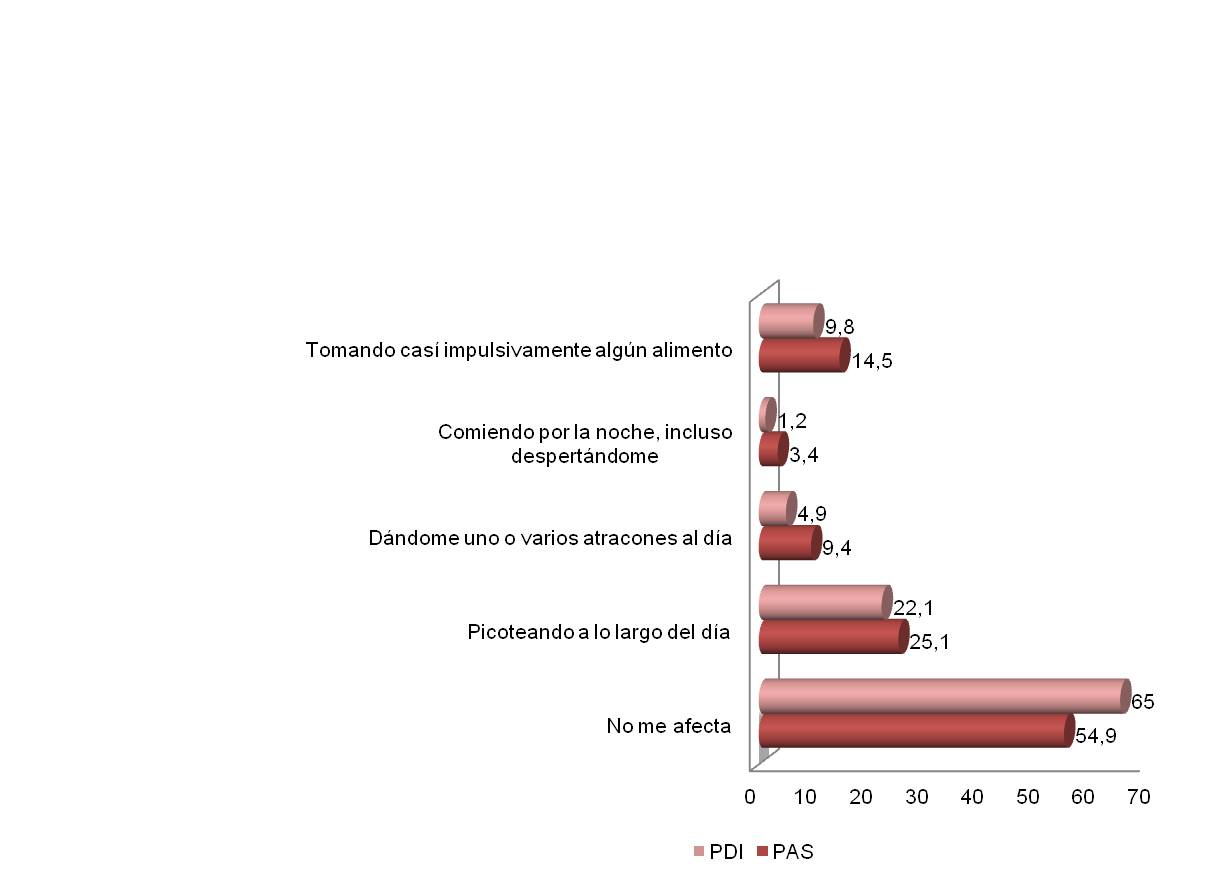
In regards to differences between the profession groups (see Figure 8), one can see that a slightly higher percentage of non-teaching personnel used these unhealthy eating patterns. Such was the case for grazing throughout the day (25.1% vs 22.1%), almost compulsively eating a food (14.5% vs 9.8%), bingeing (15.3% vs 10.4%), and night eating (3.4% vs 1.2%).
The next part of the survey included possible consequences on health from changing one’s eating pattern. Specifically, for weight, a higher percentage of women saw weight gain (25.5%) compared to men (18.2%), representing a significant difference (X2=12.514; p=.006) (See Figure 9).
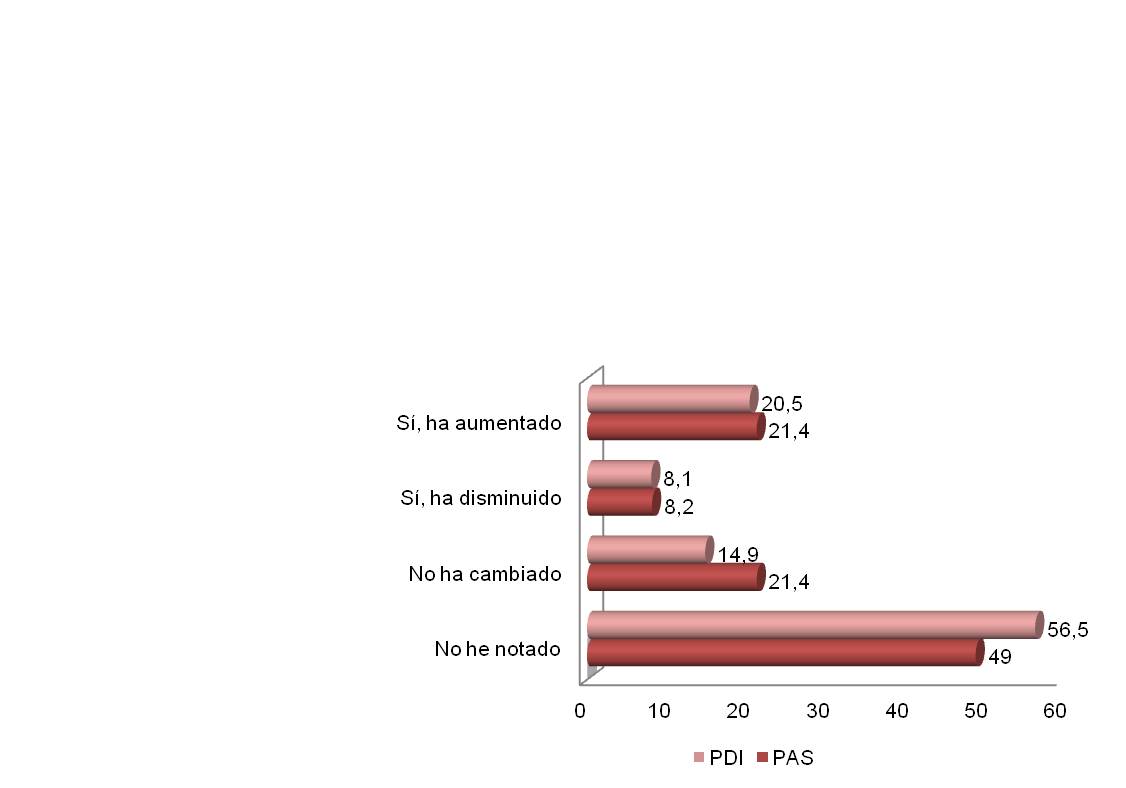
However, when comparing profession groups, the percentages were virtually the same between ASP and TRP (21.4% vs 20.5%) for people that gained weight as a consequence of changing their eating pattern, with such changes resulting from stress and negative feelings experienced in the work environment (see Figure 10).
Figure 9. Distribution of participants according to sex and fluctuations or changes in weight.
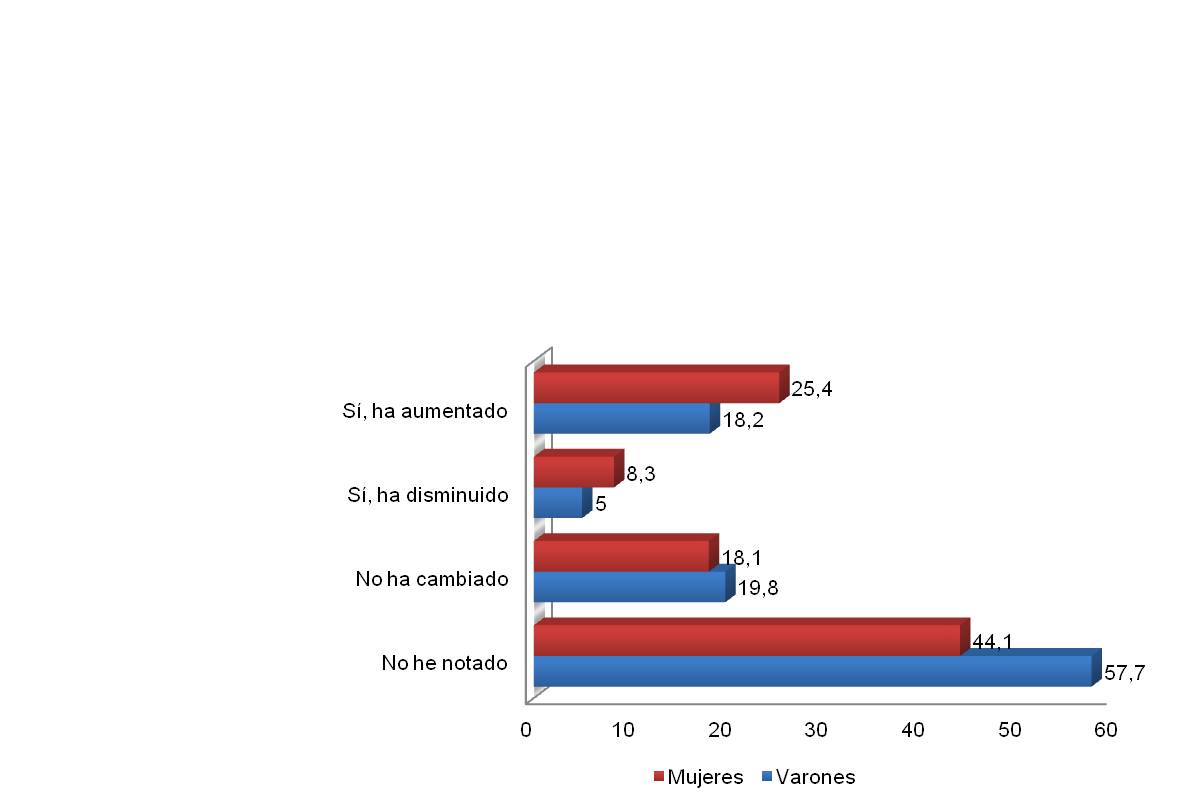
Figure 10. Distribution of participants according to profession group and fluctuations or changes in weight.
Lastly, the survey asked about any physical changes or medical problems. For differences between the sexes, a higher percentage of women complained of musculoskeletal problems (51.4% vs 42.8%) and digestive problems (23.7% vs 16.2%). However, a higher percentage of men were affected by obesity (23.4% vs 18.6%) and cardiovascular problems (16.2% vs 8.5%), and a slightly higher percentage of men had dermatological problems (11.7% vs 10.2%). There was no significant difference between men and women for any of these consequences on health (see Figure 11).
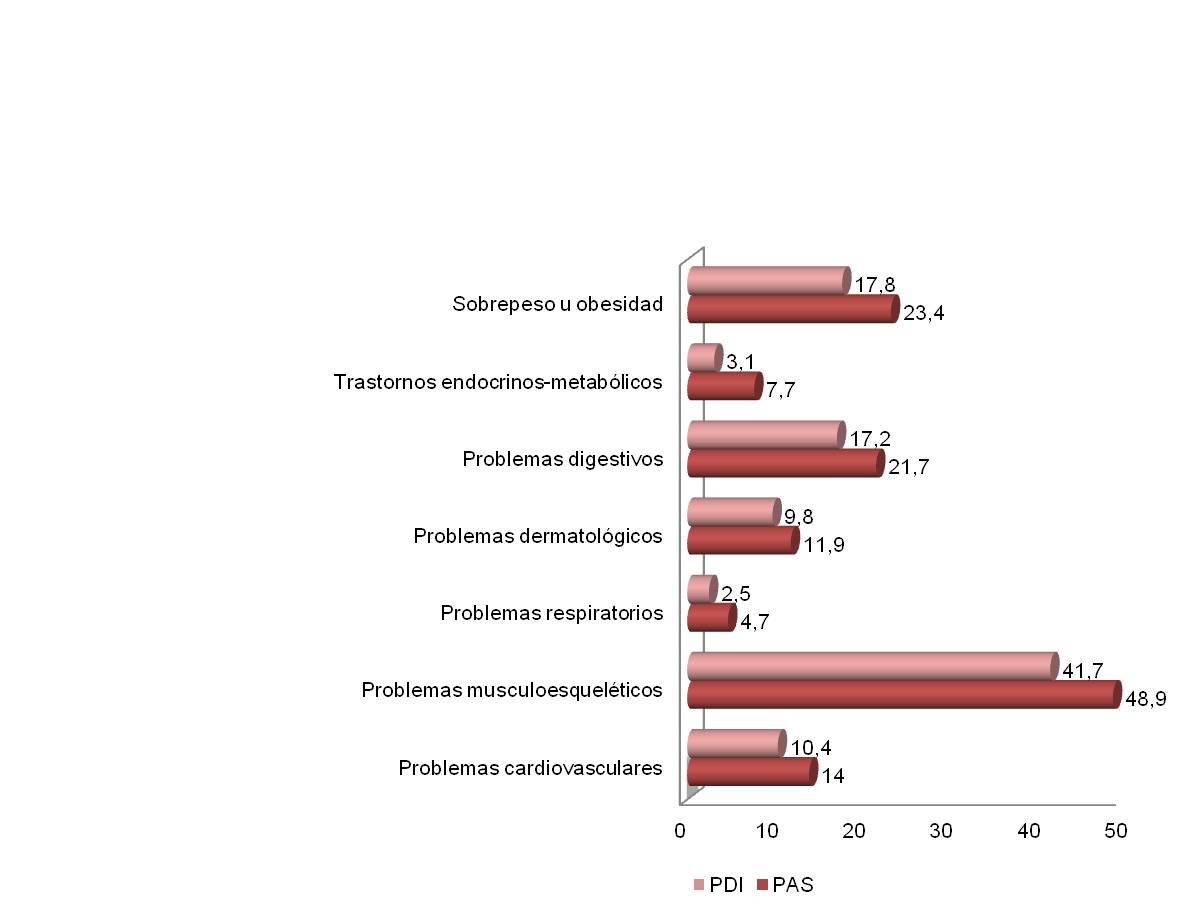
In regards to differences between profession groups, a higher percentage of non-teaching personnel saw their health affected by emotional eating that resulted from stress and negative feelings experienced in the work environment. There was a slightly higher rate of physical problems among ASP, particularly for musculoskeletal problems (48.9% vs 41.7%), digestive problems (21.7% vs 17.2%), and to a lesser extent cardiovascular problems (14% vs 10.4%) and dermatological problems (11.9% vs 9.8%), as well as overweight and obesity (23.4% vs 17.8%) (see Figure 12).
Figure 11. Physical changes or medical problems related to emotional eating according to the sex of participants.
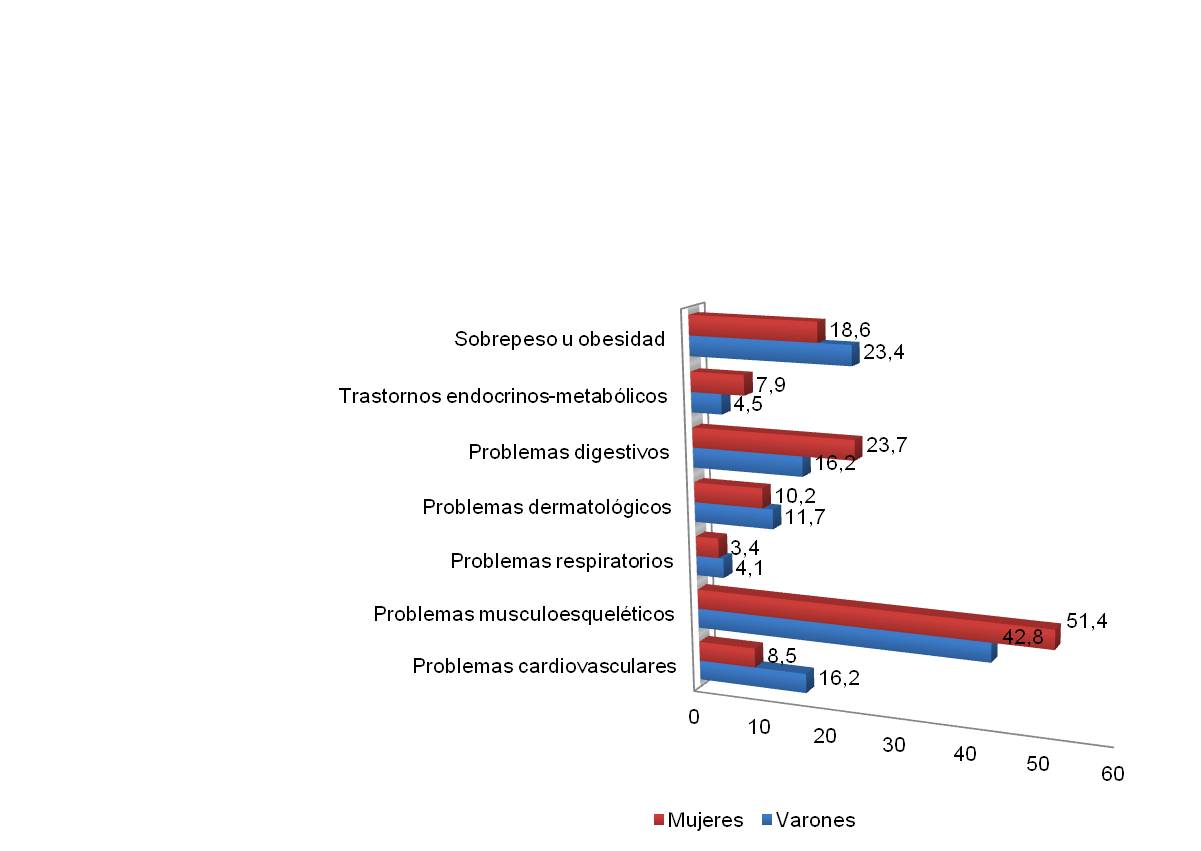
Figure 12. Physical changes or medical problems related to emotional eating according to the profession group of participants.
Discussion
In recent decades, various studies have shown that emotional eating generally occurs in reaction to negative emotions [6] and/or stress [7], with emotional eating leading to eating disorders, as well as increasing the risk of obesity when people consume foods in greater amounts or ones that are high in calories [8]. However, other studies have shown that emotional eating is not just a problem for overweight and obese people; rather, it is perceived stress that leads to emotional eating, independent of body mass index (BMI) [9].
Emotional eating is a habit considered to be a dysfunctional strategy for dealing with problems, related to regulation of emotions. On this subject, recent studies have shown that emotional eating is influenced by a combination of genetic, psychological, and emotional factors, including emotional processing, interactions with others, and strategies for dealing with problems [10]. Additionally, it is a risk factor given that, when there are stressful situations or sources of stress and tension, it can lead to the appearance or development of eating disorders such as bulimia nervosa or binge-eating disorder.
For participants in the study, the most common source of stress identified was occupational stress, notably from the organization and demands of work. On this subject, various authors [11] note that work demands are generally the top predictors for variables like emotional exhaustion or psychosomatic health problems.
Among the results of this study, it should be noted that negative emotions that lead workers to change the amount of food that they consume, i.e. eating more food or “eating their feelings”, particularly reflect feelings of anxiety: feeling anxious (42.2%), nervous (29.6%), worried (26.8%), or dissatisfied (24.8%). These results support findings from Lacey [12], who highlights that overeating due to negative moods (anger, depression, anxiety) is meant to reduce the impact of these emotions.
Recent research shows that emotional eating is more common among women, a result that was also found in this research. Specifically, women had higher percentages for the various negative emotions. Women tend to eat more when they feel bored (40.2%), dissatisfied (30.3%), depressed (29.2%), frustrated (28.8%), sad (23.7%), and to a lesser extent when they feel lacking in self-control (18.6%). However, for both men and women, feeling nervous (30.1% vs 30%) or tense (26.7% vs 27.3%) leads them to eat more with almost identical percentages. As such, negative emotions felt in stressful situations related to the work environment tend to affect the eating habits of a significant portion of workers, both men and women, in such a way that some tend to eat less and others tend to eat more. These people whose eating habits changed due to negative emotions made up a moderate percentage, with a clear trend toward eating more food for emotions related to anxiety than related to depression, especially for women.
In regards to using emotional eating as an unhealthy coping strategy, a there were slightly higher percentages of women compared to men for three of the four unhealthy eating patterns. Such was the case for night eating, almost compulsively eating a food, and grazing all day long. This pattern can be extrapolated to the general population, where we see a greater incidence of eating disorders and/or syndromes among women. In the female population, body image and dissatisfaction with one’s figure play an important role, and we see people that lack behavioral control around food. However, in our study, women had a lower percentage of BMIs indicating a health risk, i.e. indicating overweight or obesity, in spite of the fact that they were less likely to exercise or do some sort of physical activity.
In regards to profession, looking at the difference between teaching staff and non-teaching staff, negative emotions felt in stressful situations related to the work environment tend to affect the eating habits of a significant portion of workers, both teaching and non-teaching staff, in such a way that some tend to eat less and others tend to eat more. Those that try and “eat” their negative feelings, about one third of workers, find that they are affected by emotions associated both with anxiety and with mood. A slightly higher percentage of non-teaching staff engaged in these four unhealthy eating patterns, with grazing all day long and compulsively eating a food being the most common patterns in both groups of staff (ASP: 25.1% and 14.5%; TRP: 22.1% and 9.8%, respectively). Likewise, there was a higher rate of obesity for non-teaching staff (34.6%) than for teaching staff (20.6%). These differences cannot be attributed to people in the TRP group exercising more or engaging more in continuous physical activity. However, the style of work typically done by the ASP group may explain, at least partly, why people had more or less difficulty in expending energy on a daily basis, which helps maintain weight within a stable range, as the set point theory tells us.
In regards to unhealthy eating patterns used by participants, 23.9% of people tend to graze all day long and 12.3% almost compulsively eat a food. There was a lesser incidence of binge eating (7.4%), although binge eating was the abnormal pattern that produced the greatest effect on health, particularly on weight. As a consequence of these unhealthy eating habits, 45.8% of participants were overweight (15.9%) or obese (29.9%), with a markedly higher rate of overweight and obesity among men (24.1% and 36.1% respectively) than among women (5.7% and 22.3% respectively). That is to say, 60.2% for men versus 28% for women. These numbers are different from current figures for the entire Spanish population, where more than half of the adult male population is overweight or obese, as are nearly half of adult women (44.2%).
Emotional eating can be a barrier to losing weight and reducing obesity, associated with health risks such as hypertension, heart disease, digestive problems, and diabetes, among others. In this context, emotions such as sadness or anger can result in health problems like cardiovascular disease or digestive disorders. Additionally, experiencing emotions related to anxiety, such as dissatisfaction, worry, anxiousness, or nervousness, can affect sleep patterns, with a relatively high incidence of insomnia.
Two recent areas of study from scientific research that can help tackle the issues found in this study are, firstly, emotional intelligence as an adaptive coping strategy for stress to help navigate intra- and inter-personal situations [13]and, secondly, intuitive eating, which involves establishing healthy lifestyles, eliminating dieting but maintaining a healthy relationship with food [14].
Given that the team that put together this study, “Emotional eating and occupational stress: towards healthy work habits and environments”, shares this point of view, we considered it relevant, in light of the conclusions from our study that we discuss in the next section, to include the previously-mentioned most recent research with the goal of creating a protocol for intervention to promote healthy environments and habits at the University of Seville. We consider such intervention necessary to support the professions of more than 6,000 workers and 55,000 students, as an institution that is oriented towards learning and that cares about the health and well-being of the entire community, creating healthy environments and fomenting healthy lifestyles.
Conclusions
In regards to the indicator for health risk, the BMI, there was a significant percentage of overweight and obesity among workers from the U of S, with a higher rate of obesity compared to overweight. This rate is higher for men and for non-teaching staff.
In regards to the perception of stressors in daily life and in the work environment: Around half of workers perceive the work environment to be a source of stress, with higher percentages for men and teaching staff. Furthermore, a significant percentage of workers named the demands of work and how it is organized as stressors related to the work environment, with higher percentages among men and teaching staff. Additionally, to a lesser extent, the future of one’s career was considered a stressor, with similar percentages between men and women and between teaching and non-teaching staff.
In regards to the relationship between the presence of negative emotions and change in eating patterns due to stressors in the work environment:
Examining the results by sex, women tend to eat more when they feel bored, depressed, frustrated, and sad. To a lesser extent, they “eat their feelings” when they feel dissatisfied or lacking self-control. As for emotions reflecting a state of anxiety, for both men and women, feeling nervous or tense leads them to eat more, with almost identical percentages. As such, negative emotions felt in stressful situations related to the work environment tend to affect the eating habits of a significant portion of workers, both men and women, in such a way that some tend to eat less and others tend to eat more. These people whose eating habits changed due to negative emotions made up a moderate percentage, with a clear trend toward eating more food for emotions related to anxiety than related to depression, especially for women.
In regards to differences between profession groups, it was found that for both teaching and non-teaching staff, emotions related to anxiety, like feeling worried, nervous, tense, anxious, or dissatisfied, led them to eat more, with very fairly similar percentages. Additionally, for both non-teaching and teaching staff, emotions related to mood, like feeling bored, affected people’s eating habits, leading them to “eat their feelings”. For eating due to boredom, the percentage was higher for non-teaching staff. Percentages were virtually the same for feeling both depressed and sad. The ASP group tended to eat more in stressful situations where they perceived themselves as having little control. As such, negative emotions felt in stressful situations related to the work environment tend to affect the eating habits of a significant portion of workers, both teaching and non-teaching staff, in such a way that some tend to eat less and others tend to eat more. Those that try and “eat” their negative feelings, about one third of workers, find that they are affected by emotions associated both with anxiety and with mood.
In regards to how eating patterns are affected, nearly a quarter of workers tends to graze all day long. To a lesser extent, workers almost compulsively ate a particular food and had one or more binges per day. Of the four unhealthy eating patterns, the habit of “bingeing once or more per day” was the one that reflected a greater effect on health, as seen in the number of people that were overweight or obese. Breaking down the results by sex, there were slightly higher percentages of women compared to men for three of the four unhealthy eating patterns. Such was the case for night eating, almost compulsively eating a food, and grazing all day long. Men only had a higher percentage when it came to binge eating. Breaking down results by profession group, non-teaching staff had a slightly higher percentage for these four types of unhealthy patterns.
In regards to consequences for health, a higher percentage of women reported weight gain. Breaking down results by profession group, non-teaching staff and teaching staff virtually the same percentages for weight gain. Among women there was a higher percentage of people complaining of musculoskeletal and digestive problems. For men, there were higher percentages of people affected by obesity, musculoskeletal problems, and cardiovascular problems. In regards to profession group, there were slightly higher rates of health problems for the non-teaching group than for the teaching group, in particular for musculoskeletal and digestive problems, and to a lesser extent cardiovascular and dermatological problems, as well as overweight and obesity. However, there was no significant difference between men and women or between teaching and non-teaching staff for any of these health problems.
Intervention protocol for promoting healthy work environments and habits
Based on the conclusions of this study, with the goal of minimizing health problems caused by emotional eating resulting from occupational stress at the University, we consider it necessary to create healthy work environments with the following characteristics: a) multifaceted: integrated, meaning that tasks can be completed consecutively, b) stable: providing continuity throughout the year, and c) participatory: enabling interaction with other people.
In these healthy work environments, to promote worker health, we recommend offering, in general, programs that promote a) physical activity, b) healthy eating, c) weight loss, and d) stress management.
In response to the main results found in this study, guidelines from various national and international bodies, as well as the various levels where preventive action can be taken [3], in Figure 13, a series of organizational and personal measures are laid out for promoting healthy work environments and habits that would help prevent occupational stress, emotional eating, obesity, and overweight, as well as other associated health problems. These measures can be added to actions currently in place at our university from the Occupational Hazard Prevention Department [15](SEPRUS, 2015). In the next section we will elaborate on each of these measures.
Figure 13. Summary chart: Intervention protocol for promoting healthy work environments and habits.
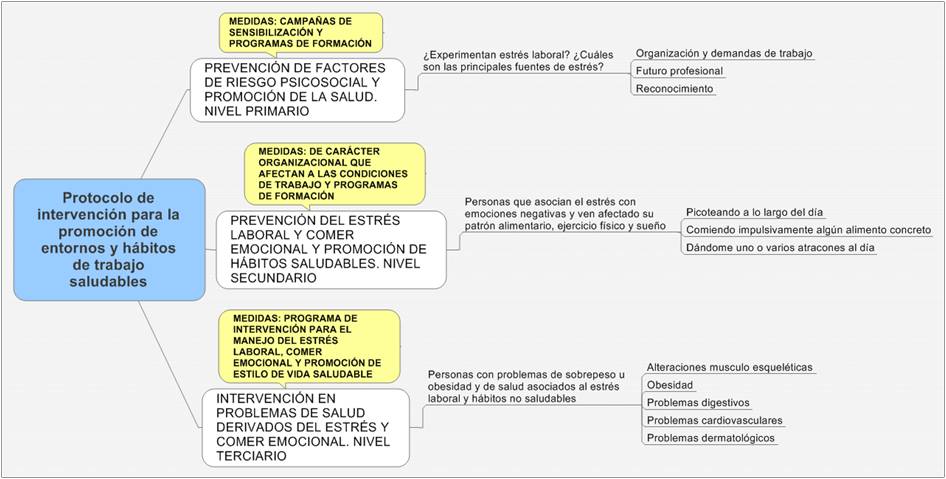
Preventing psychosocial risk factors and promoting health. First Level
a) Awareness campaigns.
Directed at the entire university community: we recommend conducting awareness campaigns that inform people about the relationship between occupational stress, emotional eating, and health, focusing on:
Promoting healthy eating: using posters and pamphlets located in the different centers and places of work, as well as next to food and drink vending machines. These posters and pamphlets should inform people of concrete steps they can take to eat healthily in the workplace.
Promote physical activity in the workplace: with posters located at elevator doors with catchy slogans like “If you can, use the stairs: your health will thank you” and at exit doors with “If you can, walk: your health will thank you”, etc.
Promote breaks that give workers personal control in moments of stress: with posters in classrooms and other workplaces with slogans that emphasize the importance of setting limits for ourselves and finding time just to breathe and re-establish emotional control. For example: “So that nothing can stop you, stop yourself and take a breather”, along with very concrete steps for calming breathing and stretches.
b) Training programs directed at management positions: “Work organization, leadership, and occupational stress: how can we contribute to creating healthy work environments?”.
Given that the main sources of stress reported by participants in our study were the organization and demands of work, the future of one’s career, and recognition of work, these trainings will be directed at university employees that hold management positions. The ideal situation would be for participation in these trainings to be mandatory, depending on how this would fit into the employees’ work schedule.
As a general objective, the trainings will aim to educate managers about the importance of having an appropriate organization of work and a leadership style for preventing and managing occupational stress, as well as about their relation to health problems in their immediate work environment. Additionally, the trainings will provide them with personal and organizational tools to help them contribute to creating healthy environments in the workplace.
The methodology used in these programs will focus on presenting relevant content and creating discussion groups to examine the viability of implementing necessary measures in the workplace.
Preventing occupational stress and promoting healthy habits. Second Level
a) Organizational measures aimed at promoting healthy eating habits, exercise, and time for rest in the workplace.
These measures can be discussed in the training courses for managers. Some possible measures would be:
Providing easy access to healthy food (fruit, healthy sandwiches, grains, water, and natural fruit juices) in the workplace. This can be done by increasing the number of vending machines in each center or through a system established in each department, office, etc.
Healthy schedules: Active anti-stress breaks that are compatible with healthy eating. We recommend a half hour without work (a rest) at mid-morning for employees that work in the morning and at mid-afternoon for employees that work in the afternoon. This would facilitate workers being able to “have a bite to eat” and do breathing and stretching exercises as recommended in the awareness campaigns.
For each center, organize yoga classes or a similar activity (days according to demand) in the morning and afternoon because of these benefits offered in terms of training one’s breathing, stretching, and toning muscles. However, these classes would bring with them a minimal financial cost for each employee, who would only have access to two classes per week so that all employees can take advantage of these classes.
Set up relaxation rooms for each department or office. If this is not possible due to space limitations, provide support for buying relaxation chairs in cases where the worker has to spend more than eight hours in the workplace at a time, whether that be because of the type of work that they do or because they cant go home to rest between morning and afternoon shifts due to distance, etc.
b) Training programs aimed at employees in general, particularly for those that may be at risk: “Occupational stress and obesity: what is emotional eating?”
These trainings will be for all university personnel, especially for those workers who feel that occupational stress is affecting their diet and weight.
As a general objective, the courses will aim to educate workers about the relationship between occupational stress and emotional eating, and about how this can affect their health. Additionally, the trainings will provide steps that can be taken to manage or deal with occupational stress and the negative emotions associated with it, as well as steps for establishing healthy lifestyle habits.
The methodology used in these programs will be psychoeducational and practical so that each participant can apply what they have learned to their personal situation.
At the end of the training programs, participants can respond to the emotional eating survey validated in this study and find out if they would be candidates for the “Intervention program: Managing occupational stress, emotional eating, and healthy lifestyles for people that are overweight or obese”, as well as find out how to access this program.
Intervention for health problems caused by occupational stress and emotional eating. Third Level
a) Intervention program aimed at overweight and obese employees, as well as employees with health problems due to unhealthy eating: “Managing occupational stress, emotional eating, and healthy lifestyles for people that are overweight or obese”.
This program will be aimed at workers that are overweight or obese or that struggle with emotional eating due to occupational stress. Workers will be selected based on the results of the survey validated in this study. If a worker is at risk, they will be eligible for the program.
The general objective of the program will be to teach workers how to manage occupational stress and emotional eating, and how to control their weight with a healthy lifestyle.
Likewise, specific objectives will include: a) reasonably lose weight, b) understand the relationship between stress and emotional eating, as well as with abnormal eating patterns, c) learn to appropriately manage negative emotions that arise from stressful situations, d) reduce negative thoughts associated with stressful situations, negative emotions, and food, e) establish healthy habits, and f) prevent health problems.
Comprehensive treatment for maintaining a healthy weight should include a combination of healthy dieting, increased physical activity, and cognitive-behavioral therapy.
Participants will work with a dietary counselor every week or every two weeks (depending on what’s convenient). This counselor will plan a diet for each participant and follow up on it. Low-calorie diets are recommended for overweight and obese people to lose weight. Each person will get an individually planned diet according to their needs. This dietary counseling and support will be provided by the health personnel from the medical office.
Likewise, it is recommended that physical activity be a part of the overall treatment for losing and maintaining weight because: a) it contributes, though modestly so, to losing weight for overweight and obese adults, b) it can reduce belly fat, c) it increases cardiopulmonary capacities, d) it can help maintain weight after some has been lost, e) it raises self-esteem and feelings of self-efficacy, and f) it prevents the occurrence of medical problems from being overweight.
Initially, participants should be encouraged to take part in moderate physical activity for 30 to 45 minutes, three to five days per week. In the long term, everyone should set the goal of getting 30 min. or more of moderate physical activity most days of the week, and preferably every day.
The psychological intervention will be done in groups (8-10 participants) in close coordination with the intervention conducted by the medical office. However, initial sessions may be conducted individually in order to conduct a more individualized evaluation of medical, psychological, and social aspects to be taken into account for creating groups that are as homogenous as possible for the intervention. Cognitive-behavioral therapy will be a useful tool as part of the treatment for reducing and maintaining weight, in combination with physical activity.
For the third-level intervention, the main techniques proposed would be: psychoeducation, stimulatory control, techniques for emotional self-control, cognitive re-structuring, and problem solving, among others. We estimate that the program can take place over about 12 sessions, occurring weekly, each about ninety minutes long. This will vary according to the development of each participant. When they achieve their set objectives, they will go through sessions for follow-up and prevention of relapses about once per month until they think that their achievements can be maintained in the long term.
Bibliography
[1] Health and Safety Executive. [En línea] http://www.hse.gov.uk/stress/.
[2] Salud, Organización Mundial de la. Ambientes de Trabajo Saludables: un modelo para la acción. Para empleadores, trabajadores, autoridades normativas y profesionales. Suiza : s.n., 2010.
[3] Burton, J. Entornos laborales saludables: fundamentos y modelo de la OMS: contextualización, prácticas y literatura de apoyo. . s.l. : World Health Organization., 2010.
[4] Condiciones de Trabajo, Burnout y Síntomas de Estrés en la Universidad: Validación de un Modelo Estructural Sobre el Efecto Mediador de la Competencia Personal Percibida. Avargues, M.L., Borda, M. y López, A. M. 2, 2010, Vol. 18.
[5] Emotional Appetite Questionnaire. Construct validity and relationship with BMI. Nolan, L. J., Halperin, L. B. y Geliebter, A. 54, 2010, Vol. 2.
[6] Emotional eating and eating disorders psychopathology. . Lindeman, M. y Stark, K. 9, 2001.
[7] Effects of distress, alexithymia and impulsivity on eating. . Van Strien, T. & Ouwens, M.A. 8, 2007.
[8] Stress and food choice. A laboratory study. . Oliver, G., Wardle, J. y Gibson, E.L. 62, 2000.
[9] BMI as a moderator of perceived stress and emotional eating in adolescents. Nguyen-Rodriguez, S.T., Chou, Ch.P., Unger, J.B. y Spruijt-Metz, D. 9, 2007.
[10] Cognitive restraint uncontrolled eating and emotional eating. DeLauson-Guillain, B., Romon, M., Musher-Eisenman, D., Heude, B., Basdevant, A. y Charles MA. 2, 2009, Vol. 5.
[11] Burnout and work engagement among teachers. Hakanen, J., Bakker, A.B. y Schaufeli, W.B. 43, 2006.
[12] Lacey, J.H. Current approaches: Bulimia nervosa. Pathogenesis. Southampton : Duphan, 1986.
[13] Emotional intelligence and emotional eating patterns: A new insight into the antecedents of eating disorders? . Zysberg, L. & Rubanov, A. 43, 2010.
[14] Intuitive eating: An emerging approach to eating behavior. . Cadena, L. y López-Guimerá, G. 31, 2015.
[15] Sevilla., Servicio de Prevención de Riesgos Laborales de la Universidad de. Guía preventiva para los empleados públicos de la Universiad de Sevilla (Edición 3ª). . Sevilla : s.n., 2015.



